The Painful Scar of the Vulva
Episiotomy, vulvar scars, and the aftermath of vaginal surgery can be painful both spontaneously and during sexual intercourse. Regenerative medicine and minimally invasive treatments can help and often provide resolution.
Non-invasive Treatments (botulinum toxin, CO2 laser, carboxytherapy)
Indication
Vulvar Pain
Surgical Technique
Botulinum Toxin, CO2 Laser, Carboxytherapy
Procedure
20 minutes
Complications
rare
Postoperative Pain
no
Recovery
immediate
Minimally Invasive Treatments
Indication
Vulvar Pain
Technique
PRP/Hyaluronic Acid
Procedure
20 minutes
Pain
no
Complications
rare
Recovery
immediate
Femifill® Vulvar Painful Scar
Indication
Painful and Retracting Scar
Surgical Technique
Adipose Tissue Harvesting, Appropriate Treatment, Multilayer Implantation of Different Adipose Preparations + CO2 Laser Vulvar
Procedure
60 /90 minutes
Complications
Rare (infections, hematomas)
Postoperative Pain
Poor if common painkillers are used
Recovery
2/4 weeks
Vulvovaginal scars can be caused by surgical procedures, traumatic events such as childbirth, or violent sexual intercourse. There are external and internal scars. External means that scars are visible on the skin of the vulva or on the mucosa of the vagina. Sometimes the scarring process is only internal when the skin and mucosa cushion the trauma better than deep tissues. This occurs classically during childbirth when, even in the presence of intact surface tissues, muscle scars and fascial plane scars can be identified. Some scars are silent, while others generate functional problems such as pain and poor tissue elasticity.
The painful outcome of episiotomy
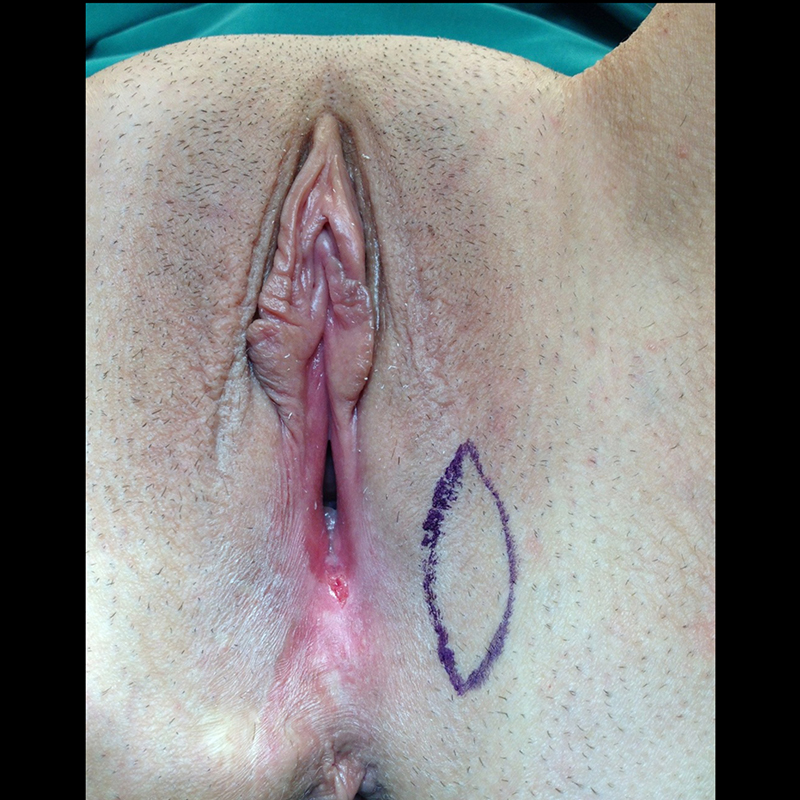
Episiotomy is a procedure performed during childbirth to prevent traumatic tearing of the vulvar walls. The National Institute of Health reports that episiotomy is performed in 58% of natural births. Episiotomy involves a cut that extends about 2 cm laterally from the vulva (mediolateral incision) or, less commonly, centrally (median incision). After childbirth, the incision is sutured. The healing process can lead to a hard and painful scar that includes fine nerve endings of the pudendal nerve, resulting in a painful scar. Sometimes it is not possible to suture the cut or torn muscles, leading to a partial loss of substance in the vulvar wall that may expose pudendal nerve filaments. The treatment of painful outcomes of episiotomy involves understanding the disrupted anatomy. Scar revision, or its removal and tissue re-suturing, is often an unsuccessful strategy. Replacing one scar with a new scar rarely produces a good result. The successful procedure we have been using for years in most cases involves implanting small amounts of adipose tissue using a particular needle that can section the scar into microfragments and soften it with the implantation of adipose tissue. Entrapped fibers are released and are no longer constrained. Tension-related pain is reduced, and often a single treatment can address the issue. In some cases where the episiotomy was vertical to the vulva and not oblique, the tissues can be so thin that they periodically ulcerate during sexual intercourse. In these cases, if the adipose tissue implantation proves insufficient, then resorting to the juxtaposition of a small flap, or tissue transposition, which acts as a patch and cushion, is considered.
The painful outcome of vaginal hysterectomy
The vaginal hysterectomy procedure is the most commonly used for the removal of the uterus. In some cases, the reconstruction of the vaginal dome results in spontaneous or exacerbated pain during penetration. The reason is attributed to the sutures of the vagina on deep tissues rich in nerve endings. In this case as well, the treatment we propose is minimally invasive and is based on the same principles outlined for episiotomy treatment. The procedure involves identifying tension points, usually identifiable as pinpoint and bilateral, and implanting a very small amount of adipose tissue injected under ultrasound guidance. Scar release leads to benefits in the majority of cases.

Perineoplasty and its scar
Perineoplasty is a procedure aimed at narrowing the perineum and the lower portion of the vulva. In some cases, rectopexy, which involves tightening the fascia lining the rectum, is combined with perineoplasty. In other cases, anterior vaginal wall plication may also be combined. When perineoplasty is performed in such a way as to reconnect the two ends of the transverse muscle, the muscle that separates from the midline postpartum, it can cause traction on the pudendal nerve, leading to irritation and pain. Lipofilling, the implantation of small amounts of adipose tissue, helps reduce neuralgia pain by scar detensioning and the anti-inflammatory action of adipose tissue.

The painful scar in aesthetic surgery procedures
Even aesthetic surgery procedures can lead to abnormal scar formation, either due to incorrect planning or execution of the procedure, the emergence of complications, or an individual tendency to develop pathological scars. Labia minora reduction should be highly respectful of the neurovascular axis, avoiding excessive reduction of the labial ridge whenever possible. The scar on the labial ridge can sometimes be bothersome as it may trap the delicate nerve endings present there. Reduction of the clitoral hood can also result in painful scars, especially if the incision lines are straight and not in a Z-shape. Creating non-straight incisions in a multiple Z-pattern is one of the secrets of plastic surgeons to achieve scars that are as soft and pliable as possible.
The first thought: away with it immediately
Scars often cause pain. The treatment philosophy should involve as the first prompt action the elimination of pain through the administration of drugs suitable for pain and inflammation management.
Regeneration and the scar
Scars can be successfully treated by the careful implantation of cell populations derived from adipose tissue. These can be implanted using a microcannula or a very thin needle, simultaneously interrupting the scar tissue and softening the tissues. Scar lipofilling and percutaneous lysis of scars have been well-known procedures in plastic surgery for over 20 years and work very well, even for vulvovaginal scars. Adipose tissue contains cells capable of inducing a process of regeneration and repair. Moreover, larger-sized cells (mature adipocytes) act as a cushion, separating the delicate nerve fibers that, when trapped in tissues, can cause pain.
When major surgery
Sometimes it is necessary to completely remove the scar tissue and replace it with healthy tissue. Almost always, the removal of a scar and direct suturing of the new margins results in an even worse scar due to the tension created on the tissues. It is then preferable to resort to the use of pedicled flaps, which bring healthy and well-vascularized tissue.

Rehabilitation
Rehabilitation after scar treatment is crucial to effectively guide the healing process. Even the best-executed scar will develop a tendency to retract, which should be countered as much as possible in the early months. Sometimes, home massage of the scar is sufficient. At times, guided massages such as those in Endermologie are helpful. When a scar is located within the vulvar or vaginal walls, the use of cones and dilators proves very useful, always recommended by a pelvic floor rehabilitation specialist.
Pre and Post